
The performance of existing buildings in earthquakes provides many lessons. Most of them – building system specific – have been very eloquently articulated in the preceding articles published in STRUCTURE (Northridge – 25 Years Later series). However, as the discussion about creating resilient communities continues, other lessons learned are factors to consider before drafting policies intended to reduce the risks associated with Natural Hazard Events (NHE).
The Hospital Seismic Retrofit Program, known as SB 1953, provides an exceptional opportunity to study a large-scale program designed to enhance seismic safety in existing buildings. Mazmanian and Sabatier (1989) studied and wrote extensively about public policy and stated that implementation runs typically through a number of stages: beginning with the passage of a statute or law, followed by policy inputs made by implementing agencies or regulations, compliance by target groups with those inputs (decisions), assessment of the actual impacts (both intended and unintended), perceived impacts of agency decisions, and, finally, important revisions or attempted revisions in the basic statute. The case of California Senate Bill (SB) 1953 provides excellent lessons in policymaking.
Legislative History
The law that established the hospital seismic retrofit program did not develop in a vacuum. Its origins lie deep within California’s concerns about earthquake safety, and it emerged from a long series of events. To truly appreciate the California Hospital Seismic Retrofit Program as a whole, it is essential to look back to the genesis of the program.
Following the 1971 San Fernando Earthquake in which several hospitals sustained substantial damage or collapsed, government officials, design professionals, and health care providers came to the realization that functioning hospitals after a major earthquake are critically important. While emergency field hospitals, medical tents, and air-lifts to available facilities are often used to supplement when hospitals are damaged, these will never provide a sufficient substitute. Only modern health care facilities, located within the damaged region and capable of functioning at full capacity, can adequately provide the needed medical assistance.
As a result, the Legislature passed the landmark Hospital Seismic Safety Act in 1972. The act required buildings to have special seismic detailing to resist earthquake forces with limited damage. Since March 7, 1973, the design, construction, and maintenance of California’s hospitals have been governed by individual statutes, regulations, and design standards aimed at assuring hospital functionality following a major earthquake. The standards are intended to ensure that vulnerable patients are safe in an earthquake, and the facilities remain functional to care for injured persons in the community after such a disaster. These standards are implemented by California’s Office of Statewide Health Planning and Development (OSHPD) and include stringent seismic design requirements, thorough plan review, approval of all designs, continuous construction inspection, materials testing, and strict monitoring of all construction projects.
However, the 1972 HSSA only applied to new hospital buildings and the alterations or remodeling of existing structures. OSHPD had no authority to require upgrading of pre-HSSA structures to meet the mandated standards for new construction. When the Act became law, it was envisioned that these pre-1973 Act or nonconforming buildings would be replaced with new conforming buildings through attrition. However, years later, a significant number of nonconforming hospital buildings with questionable earthquake performance were still in use.
The Impact of the Northridge Earthquake
The performance of these newer hospitals in the 1994 Northridge Earthquake proved that the HSSA was responsible for dramatically improving the performance of hospital buildings (Figure 1). While no buildings constructed after the HSSA were red-tagged, 24% of the pre-HSSA hospital buildings were red-tagged, meaning the buildings had to be evacuated because of structural damage. Another 33% of the pre-HSSA buildings were “yellow-tagged,” meaning the buildings had restricted use and access.
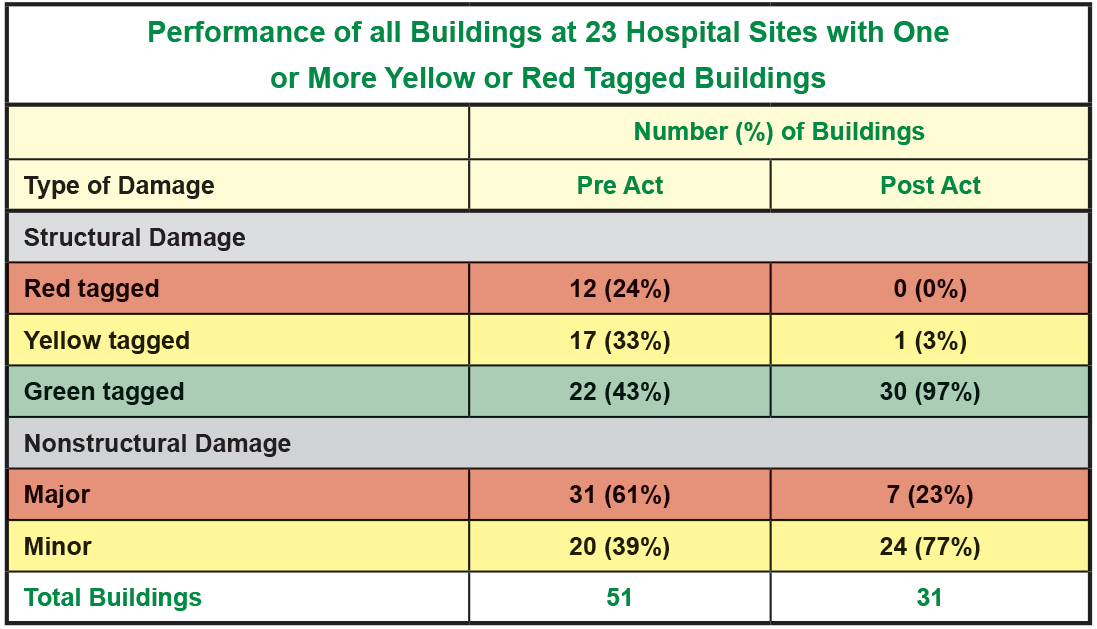
Figure 1. Northridge Earthquake – hospital performance.
The effects of the Northridge Earthquake on hospitals provided the additional incentive needed to advance legislation addressing the concern about hospital buildings built before 1973. The bill, SB 1953, was introduced into the California Senate only five weeks after the Northridge Earthquake.
The basic strategy incorporated into the SB 1953 program was first to evaluate each hospital building and place it into a specific seismic performance category (Figure 2).
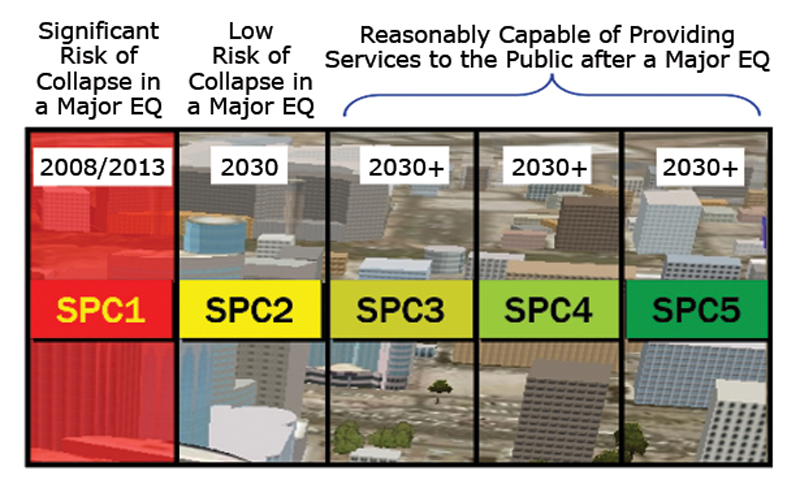
Figure 2. California hospital seismic safety definitions.
The seismic compliance portion of the law was based on a two-step approach:
- Buildings that provided acute care services and posed a significant risk of collapse during an earthquake (SPC-1 Buildings) had to be removed from service by 2008 or strengthened to SPC-2 level (LS level).
- By January 1, 2030, all acute care hospital buildings must be capable of not only surviving a major earthquake but also must be capable of providing on-going services after an earthquake.
Very rarely are public policies implemented without unanticipated, often adverse side effects, and SB1953 had its share of adverse side effects. The high percentage of SPC 1 buildings and a healthcare industry in turmoil because of financial problems, especially after the passage of the Affordable Care Act, sparked several legislative efforts to modify the original compliance deadline, which had already been extended to 2013 (Figure 3). The lesson here is that significant changes in design practice concerning existing buildings of varying ages on complicated sites take a much longer time to implement than anyone could foresee.
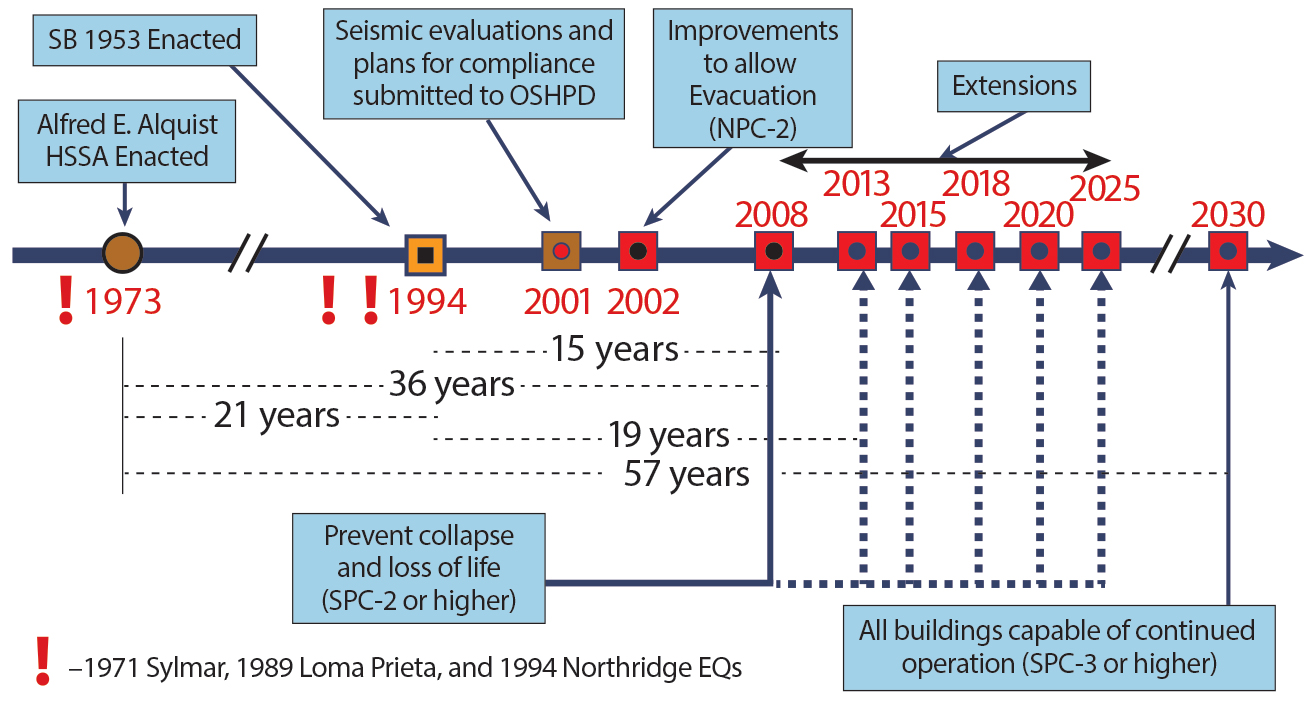
Figure 3. California hospital seismic compliance program major milestones.
Eventually, the 2008 compliance deadline was moved to 2025. However, the compliance date of 2030 for all California hospitals required to meet the “functionality” performance level has remained unchanged thus far.
Re-examine, Re-align, Repeat…
As was learned, the implementation of public policy is not a linear process. The seismic evaluation of the existing hospital buildings yielded a surprisingly large number of buildings that required either retrofit or replacement, and which constituted a large proportion of all acute care hospital buildings in California. OSHPD had to develop, in conjunction with the Hospital Building Safety Board, innovative solutions to this dilemma; “How to keep existing hospitals functioning at the same time ensuring compliance with the Law?”
OSHPD, keenly aware of the cost of retrofitting, attempted to require only the absolute minimum and gave as much flexibility as possible for compliance. OSHPD has looked for ways to lessen the impact of the seismic retrofit program without jeopardizing safety. That has been achieved by continually re-examining the program and realigning it by adopting policies to provide flexibility in its implementation, or by looking forward at the national level to adopt state of the art seismic retrofit standards to provide hospitals with options on how to meet seismic standards. The RAND (2019) corporation, in a recent report, stated: “In recent years, OSHPD has worked closely with hospitals to maintain compliance with legislative requirements of SB 1953 while pursuing opportunities to address common barriers to compliance. Such collaborative relationships between OSHPD and hospitals enable ongoing deliberation regarding the reasonableness of seismic requirements. This deliberation enhances the likelihood of identifying policy innovations that reduce the burden, and therefore increase the likelihood of compliance.”
The following are some examples of when interventions by the implementing agency (OSHPD) was very instrumental in realigning the program and facilitating compliance.
The “Safer Sooner” Concept
Why spend good money on outdated/obsolete buildings and extend life for only a few more years? In 2007, California enacted SB 306 to permit a delay in compliance for SPC-1 buildings if the hospitals demonstrated they lacked the financial capacity to remove SPC-1 buildings from service by 2013 and if the hospital agreed to replace the SPC-1 building by 2020. Twenty-four hospitals were granted SB 306 extensions.
The “Worst Buildings First” Concept
Not all buildings “posing threat to life” (SPC-1 buildings) pose the same risk. In 2005, after careful evaluation, OSHPD selected the HAZUS (Hazards US) earthquake loss estimation methodology as a tool to re-examine and assess the seismic risk for each SPC-1 hospital building (Tokas et al., 2008, 2009). Utilizing the HAZUS AEBM methodology, SPC-1 buildings were ranked based on their relative risk, thereby enabling the policymakers to implement “Worst First.”
“The Public has the Right to Know.”
In 2009, the California legislature enacted SB 499, which requires hospitals to report their compliance progress. This motivated hospitals.
Compliance Time vs. Risk
In 2011, the California legislature enacted SB 90, which authorized OSHPD to grant hospitals an extension of up to seven years beyond the 2013 deadline to retrofit or replace SPC-1 hospital buildings. The length of the extension was determined by OSHPD on a case-by-case basis using the following criteria: 1) structural integrity of the building risk (Figure 4); 2) community access to care if the hospital building was to close; and 3) financial capacity of the hospital to complete the construction projection. However, the law specifically required that such extension shall not exceed the time necessary to reasonably complete the strengthening to at least a life safety performance level (SPC-2).
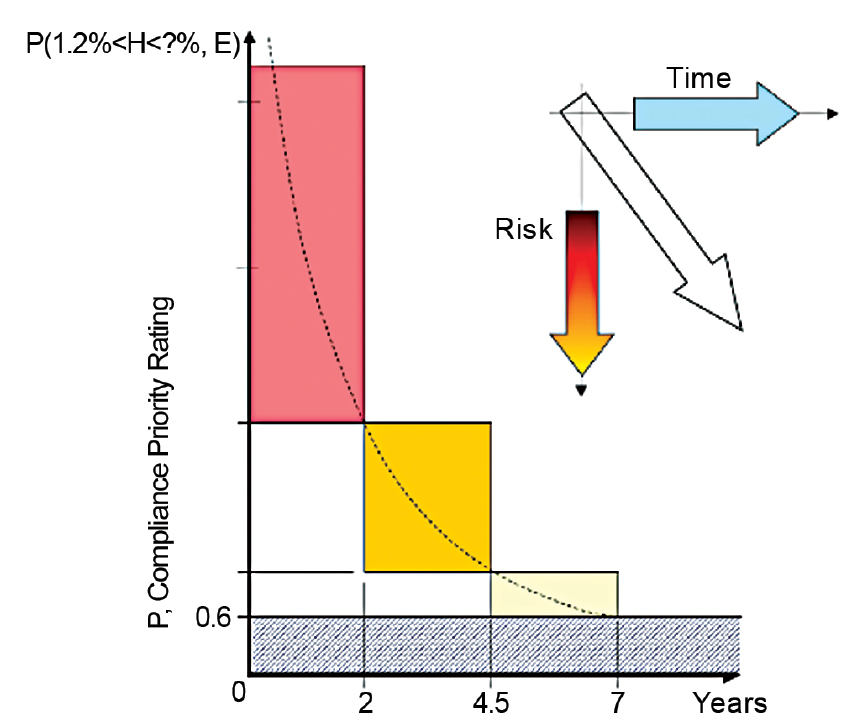
Figure 4. Compliance time vs. risk.
The Need for SPC-4D
Model codes have changed, making upgrading of pre-1973 hospital buildings to the immediate occupancy performance level cost-prohibitive to meet the 2030 functionality requirements. Rural and other hospitals in underserved areas have limited resources to upgrade to these requirements. Furthermore, the SPC-2 buildings may be landlocked by higher SPC buildings such that removing the SPC-2 building from service could make the hospital inoperable, or the hospital may not have property on which to build a replacement building.
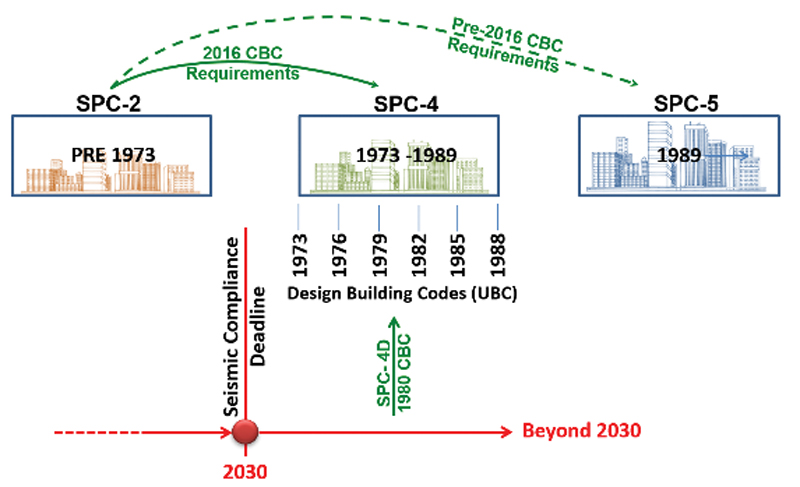
Figure 5. Seismic performance of SPC-4D hospital buildings.
As such, OSHPD instituted a new Seismic Performance Category, SPC-4D, which allows hospitals to comply with a building code edition that meets the level of performance of many SPC-4 buildings (Figure 5), but which is less than complying with current code (SPC-5) as had previously been required. Strengthening to SPC-4D is intended to control damage to permit return-to-function similar to post-1973 compliant buildings (SPC-3 or 4) but not as quickly as SPC-5 (IO level) buildings. Hospitals are using this option to strategize their master plan and explore various cost-effective options.
Policy Implementation
The extent that policies are implemented is affected by events that occur even before the policy is adopted. The need to mitigate against the likely consequences of NHE takes public regulation of private behavior to protect the public interest.
Assumptions that organizations outside the policymakers will automatically comply with directives and regulations imposed on them cannot be made. Alesch, Arendt, and Petak (2012) suggest several questions to consider before drafting a policy intended to reduce risks associated with NHE:
What are the primary obstacles to implementing public regulatory policies? How do “Organizations” make choices of how much to spend on mitigating the likely consequences of rare but potentially catastrophic events? What characteristics of public policies increase the likelihood of successful implementation? The relative long-term success of public policy design and implementation depends on the entire context within which the process takes place.
As the context changes, the policy needs to change. Rigidity in policymaking and implementation limits the capacity of the affected system to achieve the initially desired outcomes in the face of dynamic contextual change.
Following the OSHPD model, and being cognizant of the damage and disruption a major earthquake can cause for big cities and large populated areas, San Francisco and Los Angeles have led the charge in the development and successful passage of mandatory ordinances to improve the vulnerability of the building stock. Earlier voluntary retrofit programs were less effective in achieving the desired level of safety for the city. The window of discourse (otherwise known as an Overton window), which defines the range of thinking by the public on what is acceptable, sensible, or popular in terms of public safety, has shifted in public opinion and policy to make some of the voluntary retrofit programs mandatory as opinions and minds have changed over time. To achieve this required years of effort, planning, and communication with elected officials, stakeholders, and the public at large.
The Results
Following the Northridge earthquake, California hospitals have made great strides towards building and community resilience that is both practical and cost-effective. Recognizing that it is extremely costly to bring existing buildings up to the fully functional level of modern codes, OSHPD, in consultation with the Hospital Building Safety Board, has established reasonable and achievable seismic performance categories and standards for existing hospital buildings and has adapted as necessary. A majority of hospital owners have embraced the seismic safety standards and are on a path towards seismic compliance with the Hospital Seismic Safety Act. While it may appear that some of the building seismic safety standards such as SPC-4D and NPC-4D are lower than what model code dictates as the standard of performance for critical facilities, the proper enforcement of the standard compensates for it. Plan review oversight, construction observation, and continuous inspection significantly improve the reliability of hospital buildings in a damaging seismic event, which translates to re-occupancy in a very short period. California is overdue for its next big earthquake. The resiliency preparedness of the hospitals will soon be tested, and OSHPD will confirm or revise the standards based on lessons learned. Retrofitting or upgrading a building before a damaging event is always better than post-event recovery.■
References
Alesch D.J., Arendt L.A., Petak W. J., Natural Hazard Mitigation, Policy, Implementation, Organizational Choice, and Contextual Dynamics, ISBN 978-94-007-2234-7, Springer, 2012
Mazmanian DA, Sabatier PA (1989) Implementation of public policy. University of America Press, New York
Office of Statewide Health Planning and Development (1995). The Northridge Earthquake: A report to the hospital building safety board on the performance of hospitals in the Northridge Earthquake of January 17, 1994. OSHPD, Sacramento, California
Preston B. L., LaTourrette T., Broyles J. R., Briggs R. J., Catt D., Nelson C., Ringel J. S., Waxman D. A. (2019). Updating the Costs of Compliance for California’s Hospital Seismic Safety Standards. Prepared for the California Hospital Association (Sacramento, CA) by RAND Corporation, Santa Monica, CA.
Statutes, State of California, Health and Safety Code, Sections 129675-130070 seq.
Tokas C.V., Schaefer K. (1999). The Seismic Safety Program for Hospital Buildings in California, Part 1: Seismic Performance Requirements for New Hospital buildings, Workshop on Seismic Design and Retrofitting of Hospitals in Seismic Areas, Florence, Italy, October 21-22, 1999
Tokas C.V., Schaefer K. (1999). The seismic safety program for hospital buildings in California, Part 2: The seismic retrofit program for existing California hospitals. Workshop on Seismic Design and Retrofitting of Hospitals in Seismic Areas, Florence, Italy, October 21-22, 1999
Tokas C.V., Lobo R.F. (2008). Reassessment and Reprioritization of SPC-1 Hospital Building, Paper presented and published in Proceedings of the 2008 SEAOC Convention, Big Island, Hawaii, 2008, September 23 – 27
Tokas C.V., Lobo R.F. (2009). Risk-Based Seismic Evaluation of Pre 1973 Hospital Buildings Using the HAZUS Methodology, Paper presented and published in Proceedings of the ATC & SEI Conference on Improving the Seismic Performance of Existing Buildings and Other Structures, San Francisco, December 2009